Dr. A.K. Singal MBBS (Gold Medalist), DNB, MNAMS
M.CH (AIIMS, Gold Medalist)
Stecker Scholar Pediatric Urology (USA)
M.CH (AIIMS, Gold Medalist)
Stecker Scholar Pediatric Urology (USA)
A boy with urinary incontinence due to sacral agenesis finally treated by bladder augmentation using ureter (ureterocystoplasty)
Master A.T. was brought from Thane and had poor stream of urine, straining during urination and constant dribbling of urine since birth. He also had severe constipation starting at 6 months of age. The child was seen and initially managed elsewhere and underwent 3 cystoscopic surgeries for suspected urethral obstruction at some other hospital but there was no improvement. He also underwent rectal biopsy and barium enema for severe constipation but it was normal.
The child also had history of repeated severe urinary infections requiring antibiotics and he was finally referred to us during one such episode. He was 7 years of age at the time of first visit with us and he was always in diapers till this age.
Clinical evaluation showed mild weakness in foot extensors and calf muscles, the gluteal crease was short and shallow, and the buttocks were not well developed. Bulbocavernosus reflex was weak and anocutaneous reflex was also weak. Sacrum was not palpable beyond S1.
A diagnosis of sacral agenesis with neuropathic bladder was made. In view of the previous surgeries and before beginning lifelong therapy and extensive set of investigations was done.
A USG showed hydronephrosis on right side with dilated ureter and a thick-walled bladder. An MCU showed small capacity trabeculated bladder with massive Right sided VUR. The sacrum was noted to be absent beyond S1 confirming the diagnosis of partial sacral agenesis. Posterior urethra was dilated with prominent external sphincter impression (probably earlier mistaken as posterior urethral valve). Urodynamic study showed high pressure bladder with uninhibited contractions and leak at 60 ml. A DMSA scan showed a scarred poorly functioning right kidney (5%) and a normal left kidney.
A urine culture-based antibiotic was given to treat his urine infection and he did well with that. He also put on low dose antibiotic prophylaxis for prevention of infections. But most importantly he was started on CIC and anticholinergic medicine. He was able to hold urine for 1-2 hours on CIC but still had trouble and used to leak frequently. We also started bowel management program to take care of constipation. His repeat USG after 6 months showed appearance of mild hydronephrosis on left side showing increasing bladder pressures.
Considering small bladder capacity and risk of damage to the other kidney, we planned bladder augmentation surgery to give child a big bladder. Since his right kidney had hardly any function, we planned to remove the right kidney and use the dilated ureter from the right kidney for augmentation of bladder.
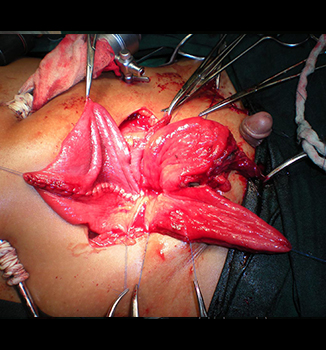
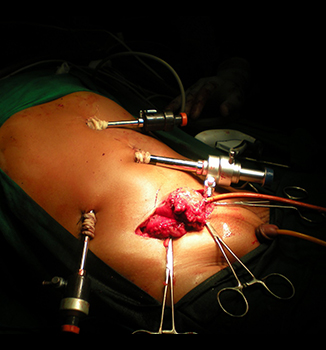
First, we did a laparoscopic right nephrectomy to avoid major pain and cut on the belly. Then we made a lower tummy incision (Pfannelstein incision) to open the bladder. From the same incision, we took out the kidney and used the ureter (20cm) to make a new bladder. Finally this new bladder made of ureter was joined to the old small bladder – Ureterocystoplasty. Child was discharged after 5 days and did very well. Now after 5 years of surgery, he is free of diapers, does catheterization (CIC) every 3-4 hours and hid left kidney is functioning well with normal renal function.
Parents are very happy as the child is free of diapers.






Dr A.K.Singal is one of the top and best pediatric urologists in India and he runs pediatric urology clinic in Navi Mumbai, Mumbai and Thane. He also personally does urodynamic study in children who need treatment for urine leak, neurogenic bladder or have bladder control issues. Dr Singal is also an expert in performing bladder augmentation surgeries for neurogenic bladder (Neuropathic bladder)
Pls fill up an enquiry form to contact his team Enquiry form